
info@beavet-medical.com
+86 19896688185

Veterinary orthopedics is a specialty that studies, diagnoses and treats cases
of traumatologies (dislocations and fractures) and pathologies related to the
bones, muscles, joints and ligaments of pets. This specialization arose
with the advancement of the veterinarian and aims to offer better treatment to
animals and provide them with pain relief and more quality of life.
Orthopedics in small animals takes care of their skeletal structure, being
considered one of the fastest growing specialties. Locomotion is part of
the pets' quality of life. These are increasingly present in world homes
and have reached a longer life expectancy. What many tutors expect is that
these animals will be able to reach old age while maintaining
well-being. Thus, there is a very high demand for orthopedic services.
Diseases of the locomotor system in dogs comprise 15% to 35% of the visits in
veterinary clinics. We know that many pets are agitated and curious and
even the most peaceful are subject to falls. Or in other situations they
may get involved in fights, being run over or suffering fractures due to old
age.
Professionals who choose to work in this area, need to know in depth about the
aspects involving bones, muscles and joints. In addition, you need to have
security to perform basic and complex surgeries.
Initial orthopedic
examinations

Orthopedics in small animals involves performing tests and techniques that will
identify the injury and the degree to which it is found. Thus, the
veterinarian will choose the most appropriate method to stabilize fractured
bones or reposition joints that have suffered an injury. The most common
complaint in offices is patients who suffer from joint diseases and usually
have an injury.
The first step in performing the exam is to assess the clinical signs of
lameness over obtaining the animal's health history. At this stage, it is
important that the animal is free to move from side to side. Thus, the
veterinarian is able to observe signs of lameness. Furthermore, possible
muscle atrophies should be checked, and if there is abnormal muscle development.
This previous analysis allows to identify which limb was affected, afterwards
it is necessary to perform the palpation on the affected limb and leave for the
exams. However, to apply the techniques safely, veterinarians need a lot
of practical experience. Only through it will it be possible to develop
surgical skills and know the most common complications in each
procedure. In the next topic, we'll talk about the tests that help with
diagnosis.
Main signs of orthopedic problems in pets
In addition to mobility difficulties, there are a number of typical signs that
can be noticed in animals with some orthopedic disease, among which we can
highlight:
Main orthopedic surgeries in dogs
Patellar dislocation is one of the most
common abnormalities affecting dogs' knees. The condition can be
congenital, also referred to as developmental, or traumatic, with dislocation
of the congenital medial patella being the most frequently observed. The
pathophysiology of congenital dislocation is not fully understood, as there is
little objective data to suggest which of the associated deformities contribute
to the induction of the dislocation and which develop as a result of patellar
dislocation.
The intensity of the deformities depends on the severity of the patellar
dislocation and the age of the animal. Another important factor is the
permanence of the dislocation; the longer the abnormal forces act on a
young dog's physical plaque, the greater the angular and torsional changes.
Clinical signs vary with the degree of dislocation and include intermittent or
consistent lameness, conformational defects, pain and reluctance to
move. The diagnosis is based on palpation of the affected knee, however
radiographic examination is useful to document the degree of limb deformity as
well as the degree of osteoarthritis present in the knee joint.
Treatment is dependent on the degree of dislocation, most of which is performed
through surgical procedures for soft and bone tissue
reconstruction. However, regardless of the techniques, the objective is to
ensure that the patella is properly positioned in the trochlear groove and,
thus, remains throughout the range of motion.
The specific etiology of patellar dislocation is not fully understood. In
most cases, the lesion is considered to be congenital or developmental, but it
can also be of traumatic origin. The history and presence of other
clinical signs, such as lacerations, abrasions, fractures, can assist in the diagnosis
of traumatic patellar dislocation. There are several surgical methods for
treating patellar dislocation and the choice depends on the severity of the
injury, or even on the surgeon's preference. Combinations of techniques
are generally performed to obtain better results. This approach was
adopted in the dogs mentioned in the present report, since, in the cases of
grades I and II, the treatment used was the technique of superimposing the
lateral retinaculum combined or not with trocleoplasty.

Additionally, the transposition of the tibial crest was performed in some grade
II knees. In the cases of grades III and IV, the methods included
overlapping the lateral retinaculum, trocleoplasty, demotomy, quadriceps
release, transposition of the tibial crest and, eventually, the fabella-patella
suture. In addition, due to the severity of the injury, in a dog with
grade IV, osteotomy of the femur was included.
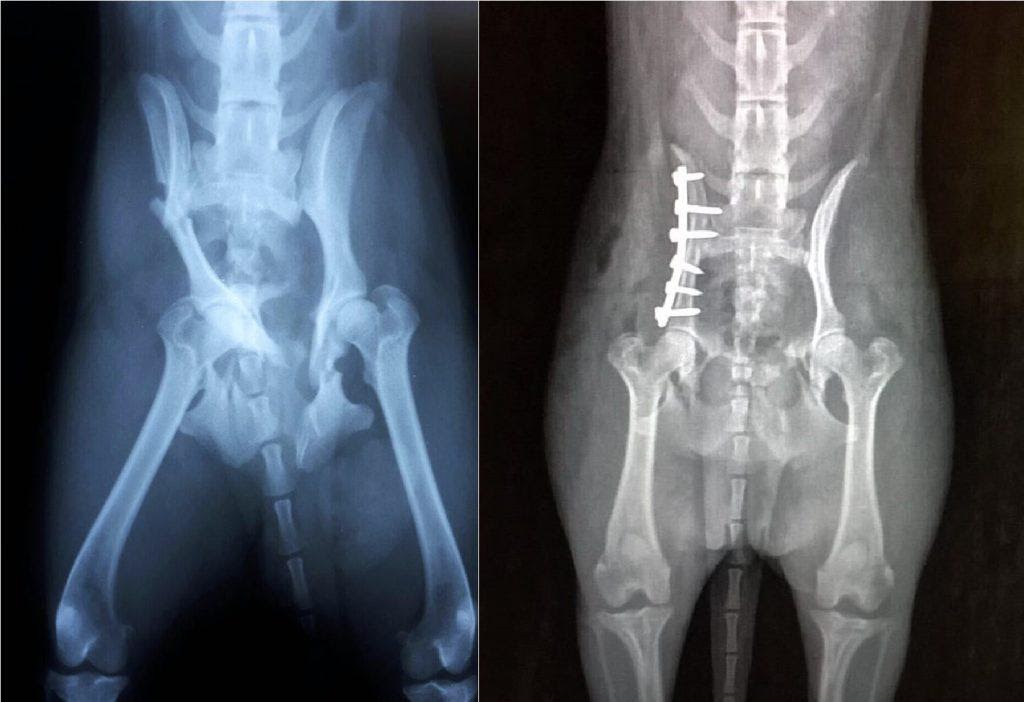
Vertebral fractures and dislocations (FLV)
are caused by traumatic or pathological injuries of the spine, resulting in
compression, laceration, concussion and / or section of neural structures.
It is considered a serious condition, due to the high risk of permanent spinal
cord damage and corresponds to approximately 7% of neurological disorders in
dogs. They are most often caused by automobile accidents. It also
occurs due to a fight between animals, kicks, falls, shocks against stationary
objects, neoplasms or vertebral infections and nutritional
osteopathies. It most frequently affects the thoracolumbar region of the
spine (T3-L3).
About 40 to 83% of patients with FLV have intercurrent lesions in other
systems.
Therefore, a thorough clinical examination is necessary to recognize these
lesions before proceeding with specific investigations. The diagnosis is
based on anamnesis, acute clinical and neurological signs and obtaining images
of the spine and spinal cord. Clinical signs range from vertebral
hyperpathy to paralysis with loss of nociception, depending on the severity of
the injury. Conservative treatment consists of the administration of
neuroprotectors, analgesics and immobilization of the spine. Surgical
treatment aims at decompression of the spinal cord, alignment of the spinal
canal, stabilization of the spine and removal of possible bone fragments from
within the spinal canal.
The prognosis depends mainly on the assessment of nociception, which indicates
the severity of the spinal cord injury, in which its presence indicates a
favorable prognosis and the absence, a prognosis reserved for the unfavorable.
Cruciate
ligament Cruciate ligaments are structures that play an
important role in the stability of the knee joint. The rupture of these is
generally associated with excessive stress on the joint, occurring most often
in young dogs of large breeds.
The rupture of the cranial cruciate ligament is one of the relatively common
conditions in the dog, having been described for the first time in 1926, and is
one of the main causes of degenerative disease of the knee joint.
The cranial cruciate ligament is the most affected, as it is primarily related
to joint movement, preventing cranial displacement of the tibia in relation to
the femur, limiting internal rotation and, consequently, knee
hyperextension. Caudal cruciate ligament rupture, although rare, is
associated with rupture of the cranial ligament.
The ligamentous lesion can be a complete rupture, with visible instability, or
partial, with secondary instability; however, both exhibit degenerative
joint changes within a few weeks. The most common mechanism of rupture of
the cranial cruciate ligament consists of a sudden rotation of the knee with
the joint in 20 ° to 50 ° of flexion, since in this position the ligaments
twist on themselves or on each other to limit the internal rotation of the
tibia in relation to the femur.
The diagnosis is based on the clinical history that reveals a picture of acute
lameness in the hind limbs, particularly during exercise. Chronic and
persistent lameness can also occur, especially in older and heavier
dogs.
To confirm the diagnosis, abnormal cranial movement of the tibia should be
checked, testing the instability of the joint with the tibia to the maximum
extent, in flexion of 15 ° to 30 ° ( Lachman Test ), and in 45
° to 90 ° of flexion, featuring the so-called "cranial drawer
signal". However, as the drawer signal is not always evident in cases
of partial rupture, in these cases, the diagnosis must be based on history and
instability with joint effusion (STROM, 1990).
Radiographic examination reveals the degree of joint involvement. Dogs
with chronic rupture of the cranial cruciate ligament develop medial thickening
of the joint capsule. Numerous techniques for repairing the ruptured
ligament have been described in the literature, following the original
technique developed by PAATSAMA (1952), who used a fascia lata flap to
reconstruct the ligament. Surgical treatment was studied by KNECHT (1976)
and since then new concepts and techniques have been introduced. Surgery
is required to stabilize joint surfaces, minimizing progressive degenerative
changes. Herniated disc

Intervertebral disc disease (DDIV) is a frequent condition in the neurological
clinic of dogs, representing 45.8% of the neurological cases treated by the
Neurology Service of the Hospital Veterinário Universitário of the Universidade
Federal de Santa Maria. The sites most affected by the disease are the
thoracolumbar (T3-L3) and cranial cervical (C1-C5) segments of the spinal cord,
occurring in 69.4% and 19.4% of cases of DDIV, respectively. Dachshunds
are 12.6 times more likely to develop DDIV than other breeds.
DDIV is rare in dogs under two years of age. In dogs of chondrodystrophic
breeds the average age varies between three and seven years and in
non-chondrodystrophic dogs, it usually varies between six and eight years of
age. Older dogs have a higher incidence of cervical DDIV. No
correlation between age and recovery of dogs with DDIV was found in some
studies, but other authors have demonstrated better and faster recovery in
young dogs.

The clinical manifestation occurs due to a combination of the compressive
effect of the disc material and the impact injury on the spinal cord, mainly
resulting from the extrusion of the disc. It varies according to the
affected spinal cord segment and the severity of the lesion, which can be
evidenced only by spinal hyperesthesia, while the more severe ones can lead to
tetraplegia / paraplegia with absence of nociception (deep pain) caudal to the
lesion.
The classification of the severity of neurological dysfunction in grades I to V
helps the clinician to issue a prognosis when assessing the patient.
The signs of neurological dysfunction for cervical and thoracolumbar DDIV are
used for classification, where: Grade I, only spinal hyperesthesia, without
neurological deficiencies; Grade II, ambulatory tetraparesis /
paraparesis; Grade III, non-ambulatory tetraparesis /
paraparesis; Grade IV, quadriplegia / paraplegia with the presence of
nociception; and Grade V, quadriplegia / paraplegia with no caudal
nociception to the lesion.
The diagnosis of DDIV is based on history and anamnesis, the lesion site defined
by neurological examination and imaging tests. Simple radiography is
hardly diagnostic for DDIV, however, in addition to excluding certain
conditions from the differential diagnosis, it is possible to notice changes
suggestive of disc disease. The accurate evaluation of spinal cord
compression requires exams such as myelography, computed tomography or magnetic
resonance imaging, making it possible to locate the
compression. Differential diagnoses include trauma, fibrocartilaginous
embolism, degenerative myelopathy, discoespondilitis, neoplasms and
meningomyelitis.
Clinical treatment for DDIV is usually indicated for dogs with hyperesthesia
associated or not with minimal neurological deficiencies and consists of
absolute rest in a cage for four to six weeks, assuming that this time would be
the minimum necessary for the repair of the fibrous annulus. Associated
with rest, opioid analgesics, muscle relaxants, steroidal and non-steroidal
anti-inflammatory drugs and physical therapy are indicated.
Surgery is the treatment of choice for dogs with severe neurological
deficiencies (non-ambulatory tetraparesis, quadriplegia, paraplegia with or
without nociception in less than 48 hours), in dogs that are refractory to
clinical treatment, or that have recurrence of the disease.
Surgical procedures vary according to the injury site and compression position,
and aim at decompression of the spinal cord. For cervical DDIV, the
ventral slot is the procedure performed routinely and dorsal laminectomy and
hemilaminectomy are less frequent. For thoracolumbar DDIV, the procedures
frequently performed are hemilaminectomy, minihemilaminectomy and
pediculectomy, associated with fenestration of the intervertebral disc

Contact: Info - Beavet Medical
Phone: +86 19896688185
Tel: +86 19896688185
Email: info@beavet-medical.com
Add: Hongkong, China
 Beavet Medical - Info
Beavet Medical - Info +86 19896688185
+86 19896688185